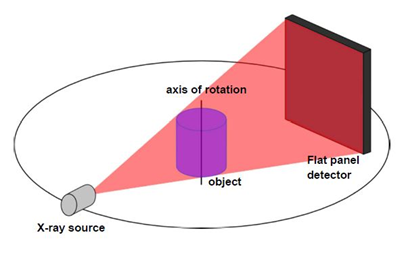
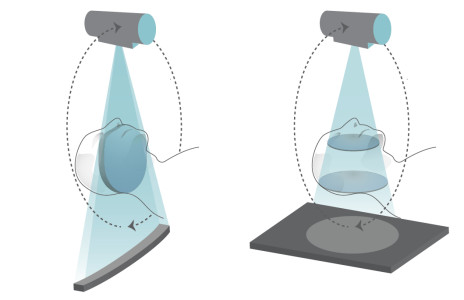
Computed Tomography is an imaging method called CT for short, it is used to prepare cross-sectional images, and the CT scanner consists of a fan-shaped x-ray tube and a set of detectors, which is an x-ray detector. It measures the output from the patient. Today, the introduction of CBCT devices with lower dose, lower cost and more accuracy in craniofacial measurements has limited the use of CT. Therefore, the use of CBCT in the clinic has increased in recent years. Medical CT differs from CBCT in terms of X-ray source detectors and reconstruction patterns. The basis of the CBCT technique is a cone beam beam focused on a two-dimensional detector. The beam handle rotates 360 degrees once and produces a series of two-dimensional images. Then these images are converted into 3D data by the complex CBCT algorithm that feld kamp et al presented in 1984. Also, CBCT is compared to Compact CT, which makes it easy to use in the dental clinic. The most important use of CBCT in the clinic includes implant surgery treatments and maxillofacial surgeries. The high accuracy of the images obtained from CBCT and the possibility of preparing three-dimensional images of the structures and the possibility of measuring on the images have led to the greater use of CBCT in many dental diagnostic and treatment matters. Although CBCT scanning is not yet used for all orthodontic treatments, however, for patients with craniofacial anomalies, pinky clefts, or in cases of orthognathic surgery, accurate CBCT images have many advantages.
CBCT has advantages over CT, which we will briefly describe.
1- X-ray limitation:
reducing the size of the radiation area by collimation of the radiation reduces the dose. CBCT has the ability to limit radiation to specific areas for specific diagnostic tasks.
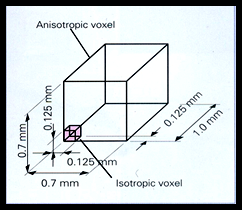
2- Image accuracy:
Since volumetric data consists of small cubic structures called voxels, their size determines the image accuracy. It is used in CT and anisotropic castles whose depth is 1-2 mm, while in CBCT and castles it is isotropic (in x, y and z dimensions are equal) and in the range between -0.4 They are located at 0.125 mm.
3- Fast image acquisition time:
Since all base images are obtained in a single CBCT rotation, the imaging time is faster.
4- Dose reduction:
The effective radiation dose of CBCT in the average range of 3.6-3.50 microsieverts is much lower than that of CT, the average range of CT is 1320-3324 microsieverts for the lower jaw and 1031-1420 microsieverts for the upper jaw.
5- Reduction of artifacts:
CBCT shows less metallic artifacts than CT.

Reconstruction of images:
The reconstructed slices are combined to create a single volumetric image, the sum of the volumetric data, the summation of all available voxels, and displayed as secondary reconstructed images in three orthogonal planes (axial, sagittal, and coronal).


Digital volumetric images can be viewed using special specialized software, these software use a technique called windowing & leveling to allow the operator to reconstruct and evaluate all the information, due to the isotropic nature of volumetric data, the data Can be cut non-orthogonally, most software provides two-dimensional non-orthogonal images, referred to as multiplanar reformation (MPR). Some types of MPR include inclined reformation, curved planar reformation, and serial transplanar reformation.
Applications of CBCT:
CBCT technology has had a major impact on jaw and face imaging. CBCT should not be considered as a replacement for panoramic or conventional radiographs, but as a complementary method for specific applications. The CBCT technique is specially designed for dentomaxillofacial imaging and has the potential to improve and improve advanced diagnoses in dentistry. The clinical use of CBCT images from the oral and maxillofacial region has increased in dentoalveolar and maxillofacial surgery, implantology, general and specialized dentistry. Perhaps the most use of CBCT is in the design of placing dental implants.
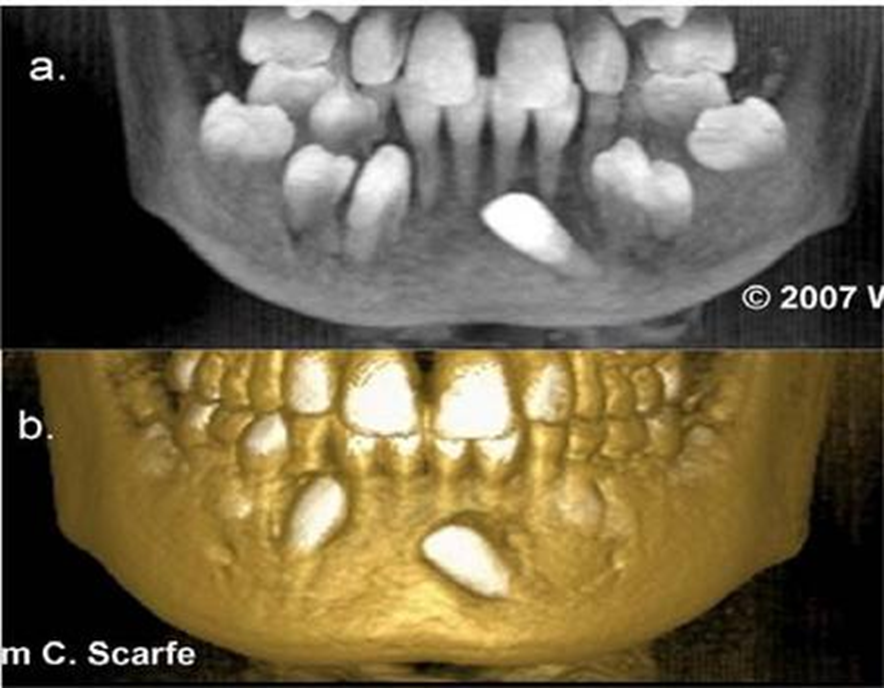
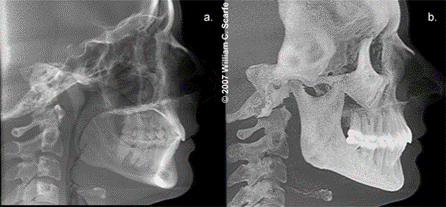
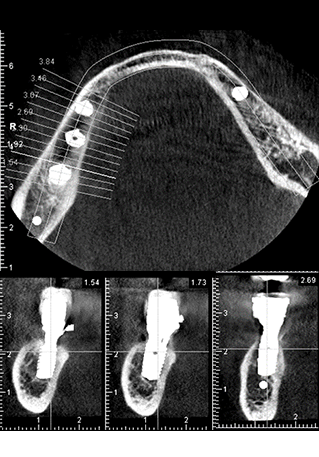
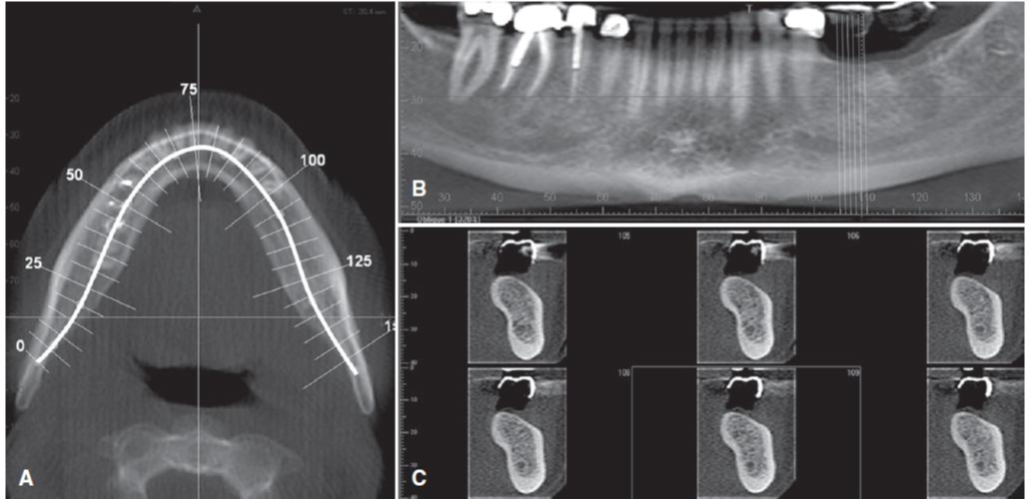
CBCT provides cross-sectional images of alveolar bone height, width and angle, and accurately delineates vital structures such as the lower alveolar neural canal in the mandible or sinus in the maxilla. CBCT imaging has been used in the diagnosis, evaluation and analysis of orthodontics and maxillofacial anomalies. CBCT shows the position of hidden and extra teeth and their relationship with the adjacent roots or other anatomical structures. Also, information can be obtained about the morphological characteristics and dimensions of the palate, tooth inclination, root analysis, and the width of the alveolar bone available for the buccolingual movement of the tooth.
CBCT provides multiplanar and three-dimensional images of the condyle and the surrounding structures to analyze and diagnose the characteristics of bone morphology, joint space and dynamic function, which are important keys to provide appropriate treatment results in patients with pain symptoms and reduced joint range of motion. to facilitate CBCT imaging can depict the characteristics of degenerative joint disease, developmental anomalies of the condyle, ankylosis, and rheumatoid arthritis. CBCT can be helpful in evaluating many jaw diseases, especially dental problems such as impacted canines, extra teeth, broken or split teeth, periapical lesions and periodontal diseases.